As we’ve previously explored in our article on global myopia epidemic, the scale of this problem rivals other major public health crises, yet it continues to receive a fraction of the attention and investment.
The global prevalence of myopia has reached unprecedented myopia levels and current projections indicate that about half of the world’s population, 5 billion people, will be myopic by 2050. Global epidemics such as obesity, deservedly attract substantial governmental action, health policy development and billion-dollar investment to tackle them. Myopia, however, remains relatively marginalised as a global public health concern. The research about childhood myopia lifestyle factors explains why prevalence is accelerating so rapidly across all populations. This may relate to a perception that myopia is simply a lifestyle inconvenience, easily managed in clinical practice, rather than a major cause of disability and socioeconomic loss.
Understanding Myopia Levels: From Low to High
Myopia is typically classified by severity of refractive error:
- Low myopia: -0.25D to -3.00D
- Moderate myopia: -3.00D to -7.00D
- High myopia: -7.00D and above
Even low myopia carries measurable risk. As the data shows, just -1.00D doubles or trebles the likelihood of serious ocular pathology.
The most important impact of myopia, in terms of public health relates to the associated risk of potentially blinding ocular pathologies. Myopic maculopathy, a condition associated with significant risks of visual loss and measurable reductions in quality of life, is the most obvious linkage between myopia and ocular pathology. This is a slowly progressive and sight threatening condition in which visual loss develops from atrophy of the retinal pigment epithelium and/or secondary complications. Far from rare, this condition is currently the third most common cause of blindness in the working age population in Ireland and the fourth commonest cause of vision impairment in the UK. In the United States, myopia is becoming increasingly prevalent, while in Beijing myopic maculopathy is the second most frequent cause of low vision. In Shanghai it is now the leading cause of blindness. The recent increases in the prevalence of myopic maculopathy documented in Asia have shown that this condition is not a specific genetic variant of myopia, but the natural consequence of any eye becoming excessively myopic.
Why There Is No “Safe” Level of Myopia
“There is no “safe” level of myopia, and even low myopia causes structural changes which put patients at increased risk of vision loss.”
Epidemiologists have also compiled an impressive array of data indicating that myopia is a highly important and an independent risk factor for a range of ocular diseases (see Figure 1). For certain conditions such as retinal detachment and myopic maculopathy, myopia appears to be the dominant risk factor and for others, e.g. cataract and glaucoma, it is second only to age. There is no “safe” level of myopia, and even low myopia causes structural changes which put patients at increased risk of vision loss. Using odds ratios, which describe the increased risk associated with being myopic relative to not having the condition, the table below shows that even 1D of myopia doubles or trebles the risk of disease, while -3.00D to -5.00D carries up to 10 times the risk of serious complications. The increased risks associated with high myopia, particularly for retinal detachment and myopic maculopathy are simply staggering.
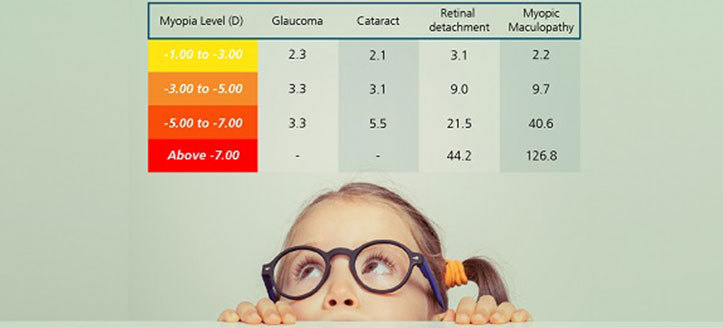
Figure 1: Relationship between level of myopia and risk of disease development. Note that even low levels of myopia carry increased risk. There is no “safe” level of myopia.
Odds ratios can be a little difficult to interpret and integrate into our discussions with patients when recommending myopia control. A patient might ask “What does ten times higher risk actually mean?”. Some clarity has been provided by researchers in the Netherlands who evaluated the prevalence of vision impairment in relation to axial length. The prevalence of vision impairment by age 75 was seen to increase substantially with increasing eye size. Among people with the longest eyeballs (over 30mm), vision impairment was almost universal, with 90% of the population affected (see Figure 2). Among people with axial length between 26-30mm, around one in every four suffer vision impairment by age 75, with those in the 28-30mm range developing vision impairment at a younger age typically compared to those in the 26-28mm range. The message is simple and clear: slowing down the abnormal growth of the eye which is characteristic of progressive myopia is hugely important for reducing risk of vision impairment.
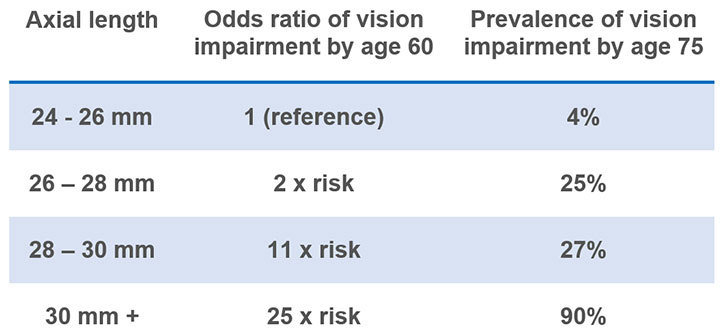
Figure 2: Prevalence of vision impairment associated with axial length in European eyes
If this is the case, why is myopia such a neglected public health priority and why is myopia control not the clinical practice norm?
Why Myopia Control Is Essential for Optometrists
The primary reason is that myopia is not widely considered to be a modifiable risk factor, yet the evidence is compelling that the use of safe and effective methods of reducing myopic progression in clinical practice would have a significant public health benefit. The same thinking is behind taking a nutritional and lifestyle approach to management of conditions like dry eye, where dietary and behavioural changes can meaningfully alter disease outcomes. The myopia management imperative is understanding that every dioptre and every fraction of a millimetre matter. Anything we can do as clinicians to reduce risk of future disease and disability will generate substantial socioeconomic and public health impact. Much of that impact depends on how successfully practitioners communicate myopia control to parents.
The time for myopia control is NOW and the place to find it should be in every optometry practice!
Conclusion
For optometrists, this evidence shifts myopia levels management from routine to being more focused on risk reduction. Accurate measurements, ongoing monitoring, and implementation of best control strategies are the foundation for patient safety. That’s why our Optometry EHR software is designed to offer better eye health management, electronic health record systems, appointments and multiple configurations to meet the specific needs of your optical business. Contact us today for free expert advice.
Recommended further reading:
- Holden BA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology 2016; 123:1036-1042
- Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog. Retin. Eye Res. 2012; 31:622-60
- Tideman JW, Snabel MC, Tedja MS et al. Association of Axial Length With Risk of Uncorrectable Visual Impairment for Europeans With Myopia. JAMA Ophthalmol. 2016;134:1355-63.